IBS is often talked about as if it were one condition-but clinically, it isn’t. IBS is divided into subtypes based on bowel habits, and those subtypes matter a lot. What helps someone with constipation-predominant IBS may worsen symptoms in diarrhea-predominant IBS. This is one of the main reasons “generic IBS advice” can feel confusing or inconsistent.
In this guide, we’ll break down IBS-C vs IBS-D vs IBS-M and how your subtype changes what tends to help-especially when it comes to diet, fiber, and medications. (For background on IBS overall, see Johns Hopkins Medicine’s overview: Irritable Bowel Syndrome (IBS).)

Why IBS subtypes matter more than most advice suggests
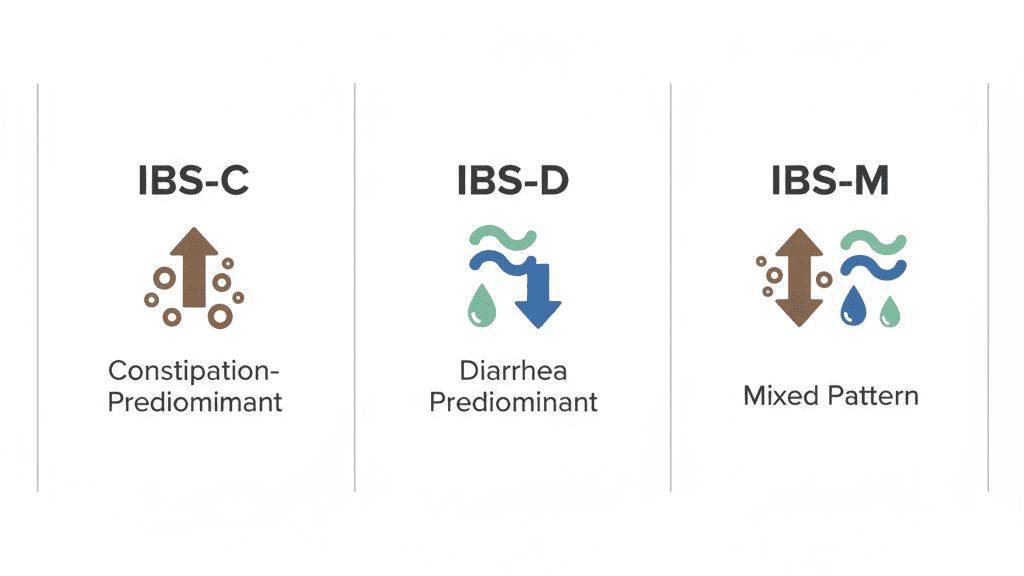
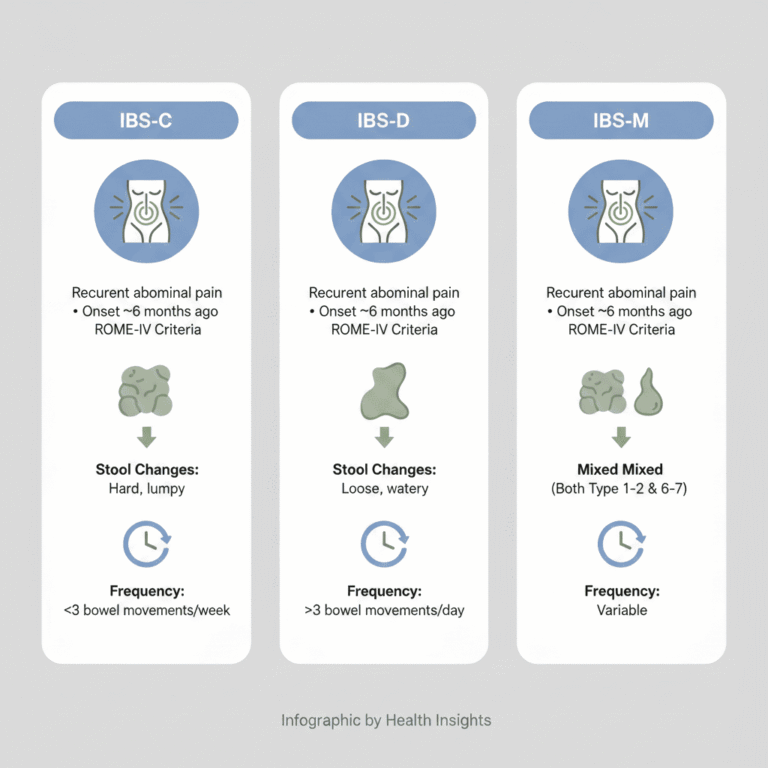
IBS is diagnosed using symptom-based criteria (Rome IV) rather than a single definitive test. Once IBS is identified, stool patterns are used to classify the subtype:
- IBS-C: constipation-predominant
- IBS-D: diarrhea-predominant
- IBS-M: mixed bowel habits
These categories are not just labels-they guide the most effective treatment choices. Cleveland Clinic provides a clear overview of IBS subtypes here: IBS types: IBS-C, IBS-D, and IBS-M.
If you want the clinical diagnostic framework, the Rome Foundation lists the Rome IV criteria here: Rome IV Criteria.
IBS-C: constipation-predominant IBS
Core symptoms
- Hard or lumpy stools
- Infrequent bowel movements
- Straining
- Bloating and abdominal discomfort
Pain in IBS-C is often linked to slowed gut motility and stool buildup-not urgency.
Diet considerations for IBS-C
Many people with IBS-C are told to “eat more fiber,” but that advice is incomplete. Helpful strategies often include:
- Regular meals (routine supports predictable motility for many people)
- Enough fluid to support stool softness
- Targeted trigger reduction (often using a low FODMAP framework when appropriate)
Important nuance: some high-FODMAP fibers can worsen bloating and pain even if constipation improves slightly. If you’re using low FODMAP strategies, Monash University is the primary research group behind the diet and offers educational resources here: Monash University Low FODMAP Diet.
Fiber: what tends to help IBS-C
Not all fiber behaves the same way. In IBS-C, soluble fiber is often better tolerated than insoluble fiber.
Often helpful:
- Soluble fiber (especially psyllium)
- Oats
Often problematic (especially if increased quickly):
- Wheat bran
- Large increases in insoluble fiber
- Big portions of raw vegetables
For evidence-based treatment direction, the American College of Gastroenterology (ACG) guideline on IBS management is here: ACG Clinical Guideline: Management of IBS.
Medications commonly used in IBS-C
Medication choices depend on severity and symptom pattern, but clinicians may consider:
- Osmotic laxatives (e.g., polyethylene glycol) for stool softening
- Secretagogues (e.g., linaclotide, plecanatide) to improve stool frequency and pain in some patients
- Neuromodulators in select cases for pain modulation
For a U.S.-focused pharmacology guideline, see the American Gastroenterological Association (AGA) guidance (covers IBS-C therapies such as linaclotide/plecanatide, among others): AGA Clinical Practice Guideline (pharmacological management).

IBS-D: diarrhea-predominant IBS
Core symptoms
- Loose or watery stools
- Urgency
- Frequent bowel movements
- Fear of accidents or needing a restroom quickly
Pain in IBS-D is often linked to rapid gut transit and gut sensitivity (visceral hypersensitivity).
Diet considerations for IBS-D
Diet strategies for IBS-D typically aim to reduce rapid fermentation, excess fluid shifts in the gut, and common triggers. A low FODMAP approach is frequently used for symptom control in IBS, particularly when it reduces excess fructose, fructans, and polyols. For an evidence-based overview, see the ACG guideline linked above.
Practical takeaway: for many people with IBS-D, choosing simpler meals and limiting “stacking” of multiple potential triggers at once makes a noticeable difference.
Fiber in IBS-D: a common source of confusion
In IBS-D, “more fiber” is not always better. The goal is often stool consistency, not stool bulk.
Often helpful:
- Small, consistent amounts of soluble fiber (like psyllium)
- Well-cooked vegetables (often easier than large raw salads)
Often problematic:
- Large amounts of insoluble fiber
- Bran-based products
- Very large raw salads
Medications commonly used in IBS-D
Depending on symptoms, clinicians may consider:
- Antidiarrheals (e.g., loperamide) primarily for stool frequency/urgency
- Antispasmodics for cramping in some patients
- Bile acid binders when bile acid diarrhea is suspected (a subset of IBS-D-like symptoms)
- Other targeted prescription options depending on patient history and risk profile
IBS-M: mixed bowel habits
Core symptoms
- Alternating constipation and diarrhea
- Unpredictable bowel patterns
- Symptoms that vary week to week
IBS-M is often the most frustrating subtype because strategies that help one phase may worsen the other. The goal is usually stability rather than aggressive symptom-chasing.
Diet considerations for IBS-M
- Prioritize consistency (meal timing, hydration, predictable foods)
- Use a structured approach if trialing low FODMAP (including reintroduction)
- Avoid extreme “fiber swings” (very low fiber one day, very high the next)
Fiber in IBS-M: moderation matters
In IBS-M, both too little and too much fiber can worsen symptoms. Many people do best with:
- Moderate, consistent soluble fiber
- Fiber spread across meals (not “all at once”)
- Gradual changes rather than sudden jumps
Medications in IBS-M
Treatment often depends on which symptom is dominant at a given time. Clinicians may adjust strategies rather than rely on a single long-term medication approach.
Why one-size-fits-all IBS advice backfires
Generic advice like “eat more fiber” or “just cut out carbs” ignores how differently IBS subtypes behave. What helps IBS-C can worsen IBS-D, and what slows diarrhea can increase constipation. Effective IBS management is subtype-aware and symptom-specific.
When symptoms change over time
IBS subtype is not always permanent. People can shift between subtypes due to stress, diet changes, medications, hormonal changes, or infections. If your symptoms change, your strategy should change too-and it may be worth discussing the shift with a clinician.
Final thoughts: your subtype changes the strategy, not the diagnosis
IBS-C, IBS-D, and IBS-M share a diagnosis-but they often require different approaches. Understanding your subtype can explain why something helped before and failed later. Better IBS management starts with matching strategies to your current symptom pattern.
References & further reading